
X-ray Computed Tomography
From Wikipedia, the free encyclopedia.
 |
| Computed tomography of human brain, from base of the skull to top. Taken with intravenous contrast medium. |
CT produces a volume of data that can be manipulated in order to demonstrate various bodily structures based on their ability to block the X-ray beam. Although, historically, the images generated were in the axial or transverse plane, perpendicular to the long axis of the body, modern scanners allow this volume of data to be reformatted in various planes or even as volumetric (3D) representations of structures. Although most common in medicine, CT is also used in other fields, such as nondestructive materials testing. Another example is archaeological uses such as imaging the contents of sarcophagi. Individuals responsible for performing CT exams are called Radiologic Technologists or Radiographers and are required to be licensed in most states.
Usage of CT has increased dramatically over the last two decades in many countries. An estimated 72 million scans were performed in the United States in 2007. One study estimated that as many as 0.4% of current cancers in the United States are due to CTs performed in the past and that this may increase to as high as 1.5-2% with 2007 rates of CT usage; however, this estimate is disputed. Kidney problems following intravenous contrast agents may also be a concern in some types of studies.
Diagnostic Use
Since its introduction in the 1970s, CT has become an important tool in medical imaging to supplement X-rays and medical ultrasonography. It has more recently been used for preventive medicine or screening for disease, for example CT colonography for patients with a high risk of colon cancer, or full-motion heart scans for patients with high risk of heart disease. A number of institutions offer full-body scans for the general population although this practice goes against the advice and official position of many professional organizations in the field.
Head
CT scanning of the head is typically used to detect infarction, tumors, calcifications, hemorrhage and bone trauma. Of the above, hypodense (dark) structures can indicate infarction and edema, hyperdense (bright) structures indicate calcifications and haemorrhage and bone trauma can be seen as disjunction in bone windows. Tumors can be detected by the swelling and anatomical distortion they cause, or by surrounding edema. Ambulances equipped with small bore multi-sliced CT scanners respond to cases involving stroke or head trauma.
 |
| Bone reconstructed in 3D |
Advantages
There are several advantages that CT has over traditional 2D medical radiography. First, CT completely eliminates the superimposition of images of structures outside the area of interest. Second, because of the inherent high-contrast resolution of CT, differences between tissues that differ in physical density by less than 1% can be distinguished. Finally, data from a single CT imaging procedure consisting of either multiple contiguous or one helical scan can be viewed as images in the axial, coronal, or sagittal planes, depending on the diagnostic task. This is referred to as multiplanar reformatted imaging.
CT is regarded as a moderate- to high-radiation diagnostic technique. The improved resolution of CT has permitted the development of new investigations, which may have advantages; compared to conventional radiography, for example, CT angiography avoids the invasive insertion of a catheter. CT Colonography (also known as Virtual Colonoscopy or VC for short) may be as useful as a barium enema for detection of tumors, but may use a lower radiation dose. CT VC is increasingly being used in the UK as a diagnostic test for bowel cancer and can negate the need for a colonoscopy.
The radiation dose for a particular study depends on multiple factors: volume scanned, patient build, number and type of scan sequences, and desired resolution and image quality. In addition, two helical CT scanning parameters that can be adjusted easily and that have a profound effect on radiation dose are tube current and pitch. Computed tomography (CT) scan has been shown to be more accurate than radiographs in evaluating anterior interbody fusion but may still over-read the extent of fusion.
Adverse Effects
Cancer
The ionizing radiation in the form of x-rays used in CT scans are energetic enough to directly or indirectly damage DNA. This and other types of DNA damage are occasionally not corrected properly by cellular repair mechanisms. Such damage to the DNA occasionally leads to cancer. The estimates of harm from CT are partly based on similar radiation exposures experienced by those present during the atomic bomb explosions in Japan during the second world war and those of nuclear industry workers.
There is a small increased risk of cancer with CT scans. It is estimated that 0.4% of current cancers in the United States are due to CTs performed in the past and that this may increase to as high as 1.5–2% with 2007 rates of CT usage; however, this estimate is disputed. This would be equivalent to one in 1000 to one in 2000 increased risk of developing a fatal cancer per 10mSv CT scan, or 29,000 new cancer cases in the United States due to the number of scans done in 2007 and 2100 new cancers in the United Kingdom. This additional risk is still low compared to the background risk of dying from cancer of ~20%. The most common cancers caused by radiation exposure are thought to be lung cancer, breast cancer, thyroid cancer, stomach cancer and leukemia.
A person's age plays a significant role in the subsequent risk of cancer. Estimated lifetime cancer mortality risks from an abdominal CT of a 1-year-old is 0.1% or 1:1000 scans. The risk for someone who is 40 years old is half that of someone who is 20 years old with substantially less risk in the elderly. The International Commission on Radiological Protection estimates that the risk to a fetus being exposed to 10 mGy (a unit of radiation exposure, see Gray (unit)) increases the rate of cancer before 20 years of age from 0.03% to 0.04% (for reference a CT pulmonary angiogram exposes a fetus to 4 mGy). A 2012 review did not find an association between medical radiation and cancer risk in children noting however the existence of limitations in the evidences over which the review is based.
CT scans can be performed with different settings for lower exposure in children with most manufacturers of CT scans as of 2007 having this function built in. Furthermore, certain conditions can require children to be exposed to multiple CT scans. Studies support informing parents of the risks of pediatric CT scanning.
Contrast
In the United States half of CT scans involve intravenously injected radiocontrast agents. The most common reactions from these agents are mild, including nausea, vomiting and an itching rash; however, more severe reactions may occur. Overall reactions occur in 1 to 3% with nonionic contrast and 4 to 12% of people with ionic contrast. Skin rashes may appear within a week to 3% of people.
The old radiocontrast agents caused anaphylaxis in 1% of cases while the newer, lower-osmolar agents cause reactions in 0.01–0.04% of cases. Death occurs in about two to 30 people per 1,000,000 administrations with newer agents being safer. When deaths do occur it is more typically in those who are female, elderly or in poor health and is secondary to either anaphylaxis or acute renal failure.
The contrast agent may induce contrast-induced nephropathy. This occurs in 2 to 7% of people who receive these agents, with greater risk in those who have preexisting renal insufficiency, preexisting diabetes, or reduced intravascular volume. People with mild kidney impairment are usually advised to ensure full hydration for several hours before and after the injection. For moderate kidney failure, the use of iodinated contrast should be avoided; this may mean using an alternative technique instead of CT. Those with severe renal failure requiring dialysis require less strict precautions, as their kidneys have so little function remaining that any further damage would not be noticeable and the dialysis will remove the contrast agent; it is normally recommended, however, to arrange dialysis as soon as possible following contrast administration to minimize any adverse effects of the contrast.
In addition to the use of intravenous contrast, orally administered contrast agents are frequently used when examining the abdomen. These are frequently the same as the intravenous contrast agents, merely diluted to approximately 10% of the concentration. However, oral alternatives to iodinated contrast exist, such as very dilute (0.5–1% w/v) barium sulfate suspensions. Dilute barium sulfate has the advantage that it does not cause allergic-type reactions or kidney failure, but cannot be used in patients with suspected bowel perforation or suspected bowel injury, as leakage of barium sulfate from damaged bowel can cause fatal peritonitis.
Scan Dose
The reports show average radiation exposures, however, there is a wide variation in radiation doses between similar scan types, where the highest dose could be as much as 22 times higher than the lowest dose. A typical plain film x-ray involves radiation dose of 0.01 to 0.15 mGy, while a typical CT can involve 10–20 mGy for specific organs, and can go up to 80 mGy for certain specialized CT scans.
For purposes of comparison, the world average dose rate from naturally occurring sources of background radiation is 2.4 mSv per year, equal for practical purposes in this application to 2.4 mGy per year. While there is some variation, most people (99%) received less than 7 mSv per year as background radiation. Medical imaging as of 2007 accounted for half of the radiation exposure of those in the United States with CT scans making up two thirds of this amount. In the United Kingdom it accounts for 15% of radiation exposure. The average radiation dose from medical sources is ~0.6 mSv per person globally as of 2007. Those in the nuclear industry in the United States are limited to doses of 50 mSv a year and 100 mSv every 5 years.
Radiation Dose Units
The radiation dose reported in the gray or mGy unit is proportional to the amount of energy that the irradiated body part is expected to absorb, and the physical effect (such as DNA double strand breaks) on the cells' chemical bonds by x-ray radiation is proportional to that energy.
The sievert unit is used in the report of the effective dose. The sievert unit in the context of CT scans, does not correspond to the actual radiation dose that the scanned body part absorbs, but rather to another radiation dose of another scenario, in which the whole body absorbs the other radiation dose, and where the other radiation dose is of a magnitude that is estimated to have the same probability to induce cancer as the CT scan. Thus, as is shown in the table above, the actual radiation that is absorbed by a scanned body part is often much larger than the effective dose suggests. A specific measure, termed the computed tomography dose index (CTDI), is commonly used as an estimate of the radiation absorbed dose for tissue within the scan region, and is automatically computed by medical CT scanners.
The equivalent dose is the effective dose of a case, in which the whole body would actually absorb the same radiation dose, and the sievert unit is used in its report. In the case of non-uniform radiation, or radiation given to only part of the body, which is common for CT examinations, using the local equivalent dose alone would overstate the biological risks to the entire organism.
Excess Doses
In October, 2009, the US Food and Drug Administration (FDA) initiated an investigation of brain perfusion CT (PCT) scans, based on overdoses of radiation caused by incorrect settings at one particular facility for this particular type of CT scan. Over 256 patients over an 18 month period were exposed, over 40% lost patches of hair, and prompted the editorial to call for increased CT quality assurance programs, while also noting that "while unnecessary radiation exposure should be avoided, a medically needed CT scan obtained with appropriate acquisition parameter has benefits that outweigh the radiation risks." Similar problems have been reported at other centers. These incidents are believed to be due to human error.
Campaigns
In response to increased concern by the public and the ongoing progress of best practices, The Alliance for Radiation Safety in Pediatric Imaging was formed within the Society for Pediatric Radiology. In concert with The American Society of Radiologic Technologists, The American College of Radiology and The American Association of Physicists in Medicine, the Society for Pediatric Radiology developed and launched the Image Gently Campaign which is designed to maintain high quality imaging studies while using the lowest doses and best radiation safety practices available on pediatric patients. This initiative has been endorsed and applied by a growing list of various professional medical organizations around the world and has received support and assistance from companies that manufacture equipment used in Radiology.
Following upon the success of the Image Gently campaign, the American College of Radiology, the Radiological Society of North America, the American Association of Physicists in Medicine and the American Society of Radiologic Technologists have launched a similar campaign to address this issue in the adult population called Image Wisely.
The World Health Organization and International Atomic Energy Agency (IAEA) of the United Nations have also been working in this area and have ongoing projects designed to broaden best practices and lower patient radiation dose.
Prevalence
Usage of CT has increased dramatically over the last two decades. An estimated 72 million scans were performed in the United States in 2007. Of these, six to eleven percent are done in children, an increase of seven to eightfold from 1980. Similar increases have been seen in Europe and Asia. In Calgary, Canada 12.1% of people who present to the emergency with an urgent complaint received a CT scan, most commonly either of the head or of the abdomen. The percentage who received CT, however, varied markedly by the emergency physician who saw them from 1.8% to 25%. In the emergency department in the United States, CT or MRI imaging is done in 15% of people who present with injuries as of 2007 (up from 6% in 1998).
The increased use of CT scans has been the greatest in two fields: screening of adults (screening CT of the lung in smokers, virtual colonoscopy, CT cardiac screening, and whole-body CT in asymptomatic patients) and CT imaging of children. Shortening of the scanning time to around 1 second, eliminating the strict need for the subject to remain still or be sedated, is one of the main reasons for the large increase in the pediatric population (especially for the diagnosis of appendicitis). As of 2007 in the United States a proportion of CT scans are performed unnecessarily. Some estimates place this number at 30%. There are a number of reasons for this including: legal concerns, financial incentives, and desire by the public. There is also otherwise healthy people receiving full body CT scans as screening for which there is no evidence to support.
Process
X-ray slice data is generated using an X-ray source that rotates around the object; X-ray sensors are positioned on the opposite side of the circle from the X-ray source. The earliest sensors were scintillation detectors, with photomultiplier tubes excited by (typically) cesium iodide crystals. Cesium iodide was replaced during the 1980s by ion chambers containing high-pressure Xenon gas. These systems were in turn replaced by scintillation systems based on photodiodes instead of photomultipliers and modern scintillation materials (for example rare earth garnet or rare earth oxide ceramics) with more desirable characteristics.
Initial machines would rotate the X-ray source and detectors around a stationary object. Following a complete rotation, the object would be moved along its axis, and the next rotation started. Newer machines permitted continuous rotation with the object to be imaged slowly and smoothly slid through the X-ray ring. These are called helical or spiral CT machines. A subsequent development of helical CT was multi-slice (or multi-detector) CT; instead of a single row of detectors, multiple rows of detectors are used effectively capturing multiple cross-sections simultaneously. Systems with a very large number of detector rows, such that the z-axis coverage is comparable to the xy-axis coverage are often termed cone beam CT, due to the shape of the X-ray beam (strictly, the beam is pyramidal in shape, rather than conical).
In conventional CT machines, an X-ray tube and detector are physically rotated behind a circular shroud (see the image above right). An alternative, short lived design, known as electron beam tomography (EBT), used electromagnetic deflection of an electron beam within a very large conical X-ray tube and a stationary array of detectors to achieve very high temporal resolution, for imaging of rapidly moving structures, for example the coronary arteries. Cone-beam CT functionality is also an increasingly common function found in medical fluoroscopy equipment; by rotating the fluoroscope around the patient, a geometry similar to CT can be obtained, and by treating the 2D X-ray detector in a manner similar to a CT detector with a massive number of rows, it is possible to reconstruct a 3D volume from a single rotation using suitable software.
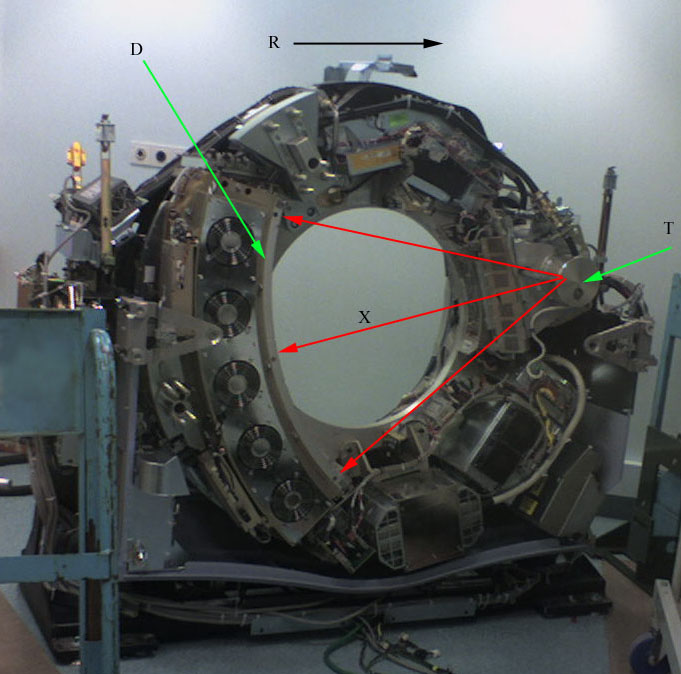 |
CT scanner with cover removed to show
internal components. Legend:
T: X-ray tube
D: X-ray detectors
X: X-ray beam
R: Gantry rotation
|
A visual representation of the raw data obtained is called a sinogram, yet it is not sufficient for interpretation. Once the scan data has been acquired, the data must be processed using a form of tomographic reconstruction, which produces a series of cross-sectional images. In terms of mathematics, the raw data acquired by the scanner consists of multiple "projections" of the object being scanned. These projections are effectively the Radon transformation of the structure of the object. Reconstruction, essentially involves solving the inverse Radon transformation.
The technique of filtered back projection is one of the most established algorithmic techniques for this problem. It is conceptually simple, tunable and deterministic. It is also computationally undemanding, with modern scanners requiring only a few milliseconds per image. However, this is not the only technique available: the original EMI scanner solved the tomographic reconstruction problem by linear algebra, but this approach was limited by its high computational complexity, especially given the computer technology available at the time. More recently, manufacturers have developed iterative physical model-based maximum likelihood expectation maximization techniques. These techniques are advantageous because they use an internal model of the scanner's physical properties and of the physical laws of X-ray interactions. Earlier methods, such as filtered back projection, assume a perfect scanner and highly simplified physics, which leads to a number of artifacts, high noise and impaired image resolution. Iterative techniques provide images with improved resolution, reduced noise and fewer artifacts, as well as the ability to greatly reduce the radiation dose in certain circumstances. The disadvantage is a very high computational requirement, but advances in computer technology and high-performance computing techniques, such as use of highly parallel GPU algorithms, now allow practical use.
Pixels in an image obtained by CT scanning are displayed in terms of relative radiodensity. The pixel itself is displayed according to the mean attenuation of the tissue(s) that it corresponds to on a scale from +3071 (most attenuating) to −1024 (least attenuating) on the Hounsfield scale. Pixel is a two dimensional unit based on the matrix size and the field of view. When the CT slice thickness is also factored in, the unit is known as a Voxel, which is a three-dimensional unit. The phenomenon that one part of the detector cannot differentiate between different tissues is called the "Partial Volume Effect". That means that a big amount of cartilage and a thin layer of compact bone can cause the same attenuation in a voxel as hyperdense cartilage alone. Water has an attenuation of 0 Hounsfield units (HU), while air is −1000 HU, cancellous bone is typically +400 HU, cranial bone can reach 2000 HU or more (os temporale) and can cause artifacts. The attenuation of metallic implants depends on atomic number of the element used: Titanium usually has an amount of +1000 HU, iron steel can completely extinguish the X-ray and is, therefore, responsible for well-known line-artifacts in computed tomograms. Artifacts are caused by abrupt transitions between low- and high-density materials, which results in data values that exceed the dynamic range of the processing electronics.
Contrast mediums used for X-ray CT, as well as for plain film X-ray, are called radiocontrasts. Radiocontrasts for X-ray CT are, in general, iodine-based. Often, images are taken both with and without radiocontrast. CT images are called precontrast or native-phase images before any radiocontrast has been administrated, and postcontrast after radiocontrast administration.
Two-dimensional CT images are conventionally rendered so that the view is as though looking up at it from the patient's feet. Hence, the left side of the image is to the patient's right and vice versa, while anterior in the image also is the patient's anterior and vice versa. This left-right interchange corresponds to the view that physicians generally have in reality when positioned in front of patients.
CT data sets have a very high dynamic range which must be reduced for display or printing. This is typically done via a process of "windowing", which maps a range (the "window") of pixel values to a greyscale ramp. For example, CT images of the brain are commonly viewed with a window extending from 0 HU to 80 HU. Pixel values of 0 and lower, are displayed as black; values of 80 and higher are displayed as white; values within the window are displayed as a grey intensity proportional to position within the window. The window used for display must be matched to the X-ray density of the object of interest, in order to optimize the visible detail.
Three-dimensional Reconstruction
Because contemporary CT scanners offer isotropic or near isotropic, resolution, display of images does not need to be restricted to the conventional axial images. Instead, it is possible for a software program to build a volume by "stacking" the individual slices one on top of the other. The program may then display the volume in an alternative manner.
Multiplanar Reconstruction
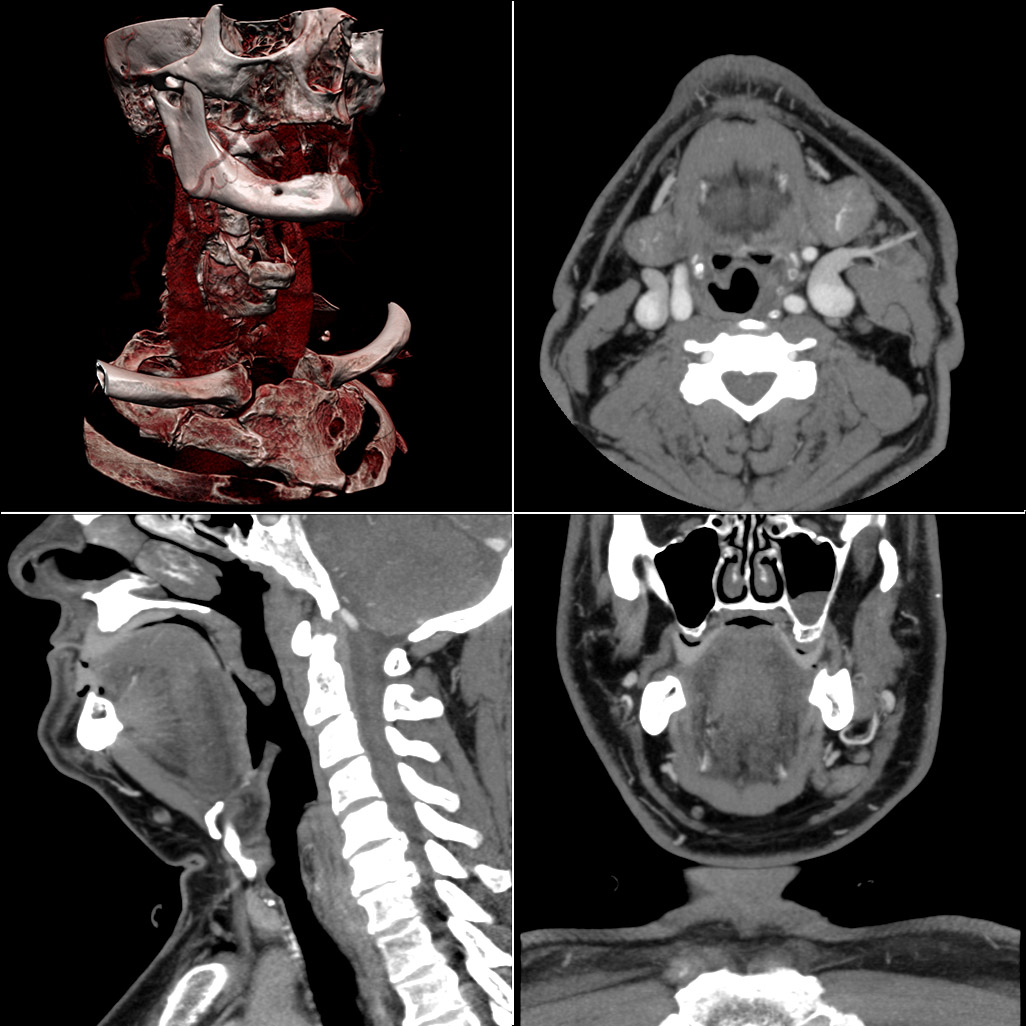 |
Typical screen layout for diagnostic software,
showing one 3D and three MPR views
|
MPR is frequently used for examining the spine. Axial images through the spine will only show one vertebral body at a time and cannot reliably show the intervertebral discs. By reformatting the volume, it becomes much easier to visualise the position of one vertebral body in relation to the others.
Modern software allows reconstruction in non-orthogonal (oblique) planes so that the optimal plane can be chosen to display an anatomical structure. This may be particularly useful for visualising the structure of the bronchi as these do not lie orthogonal to the direction of the scan.
For vascular imaging, curved-plane reconstruction can be performed. This allows bends in a vessel to be "straightened" so that the entire length can be visualised on one image, or a short series of images. Once a vessel has been "straightened" in this way, quantitative measurements of length and cross sectional area can be made, so that surgery or interventional treatment can be planned.
MIP reconstructions enhance areas of high radiodensity, and so are useful for angiographic studies. MIP reconstructions tend to enhance air spaces so are useful for assessing lung structure.
3D Rendering Techniques
Surface Rendering
A threshold value of radiodensity is set by the operator (e.g., a level that corresponds to bone). From this, a three-dimensional model can be constructed using edge detection image processing algorithms and displayed on screen. Multiple models can be constructed from various thresholds, allowing different colors to represent each anatomical component such as bone, muscle, and cartilage. However, the interior structure of each element is not visible in this mode of operation.
Volume Rendering
Surface rendering is limited in that it will display only surfaces that meet a threshold density, and will display only the surface that is closest to the imaginary viewer. In volume rendering, transparency, colors and shading are used to allow a better representation of the volume to be shown in a single image. For example, the bones of the pelvis could be displayed as semi-transparent, so that, even at an oblique angle, one part of the image does not conceal another.
Image Segmentation
Where different structures have similar radiodensity, it can become impossible to separate them simply by adjusting volume rendering parameters. The solution is called segmentation, a manual or automatic procedure that can remove the unwanted structures from the image.
Image Quality
Artifacts
Although images produced by CT are generally faithful representations of the scanned volume, the technique is susceptible to a number of artifacts, such as the following: Chapters 3 and 5.
Streak Artifact
Streaks are often seen around materials that block most X-rays, such as metal or bone. Numerous factors contribute to these streaks: undersampling, photon starvation, motion, beam hardening, and Compton scatter. This type of artifact commonly occurs in the posterior fossa of the brain, or if there are metal implants. The streaks can be reduced using newer reconstruction techniques or approaches such as metal artifact reduction (MAR).
Partial Volume Effect
This appears as "blurring" of edges. It is due to the scanner being unable to differentiate between a small amount of high-density material (e.g., bone) and a larger amount of lower density (e.g., cartilage). The reconstruction assumes that the X-ray attenuation within each voxel is homogenous; this may not be the case at sharp edges. This is most commonly seen in the z-direction, due to the conventional use of highly anisotropic voxels, which have a much lower out-of-plane resolution, than in-plane resolution. This can be partially overcome by scanning using thinner slices, or an isotropic acquisition on a modern scanner.
Ring Artifact
Probably the most common mechanical artifact, the image of one or many "rings" appears within an image. This is usually due to a detector fault, or miscalibration of an individual detector element.
Noise
This appears as grain on the image and is caused by a low signal to noise ratio. This occurs more commonly when a thin slice thickness is used. It can also occur when the power supplied to the X-ray tube is insufficient to penetrate the anatomy.
Motion Artifact
This is seen as blurring and/or streaking, which is caused by movement of the object being imaged. Motion blurring might be reduced using a new technique called IFT (incompressible flow tomography).
Windmill
Streaking appearances can occur when the detectors intersect the reconstruction plane. This can be reduced with filters or a reduction in pitch.
Beam Hardening
This can give a "cupped appearance". It occurs when there is more attenuation along a path passing through the center of an object, than a path that grazes the edge. This is easily corrected by filtration and software.
Dose vs. Image Quality
An important issue within radiology today is how to reduce the radiation dose during CT examinations without compromising the image quality. In general, higher radiation doses result in higher-resolution images, while lower doses lead to increased image noise and unsharp images. However, increased dosage raises increase the adverse side effects, including the risk of radiation induced cancer – a four-phase abdominal CT gives the same radiation dose as 300 chest x-rays (See the Scan dose section). Several methods that can reduce the exposure to ionizing radiation during a CT scan exist.
- New software technology can significantly reduce the required radiation dose.
- Individualize the examination and adjust the radiation dose to the body type and body organ examined. Different body types and organs require different amounts of radiation.
- Prior to every CT examination, evaluate the appropriateness of the exam whether it is motivated or if another type of examination is more suitable. Higher resolution is not always suitable for any given scenario, such as detection of small pulmonary masses.
History
Origins of Tomography
 |
| The prototype CT scanner |
Mathematical Theory
The mathematical theory behind the tomographic reconstruction dates back to 1917 where the invention of Radon Transform by an Austrian mathematician Johann Radon. He showed mathematically that a function could be reconstructed from an infinite set of its projections. In 1937, a Polish mathematician, named Stefan Kaczmarz, developed a method to find an approximate solution to a large system of linear algebraic equations. This led the foundation to another powerful reconstruction method called "Algebraic Reconstruction Technique (ART)" which was later adapted by Sir Godfrey Hounsfield as the image reconstruction mechanism in his famous invention, the first commercial CT scanner.
In 1956, Ronald N. Bracewell used a method similar to the Radon Transform to reconstruct a map of solar radiation from a set of solar radiation measurements. In 1959, William Oldendorf, a UCLA neurologist and senior medical investigator at the West Los Angeles Veterans Administration hospital, conceived an idea for "scanning a head through a transmitted beam of X-rays, and being able to reconstruct the radiodensity patterns of a plane through the head" after watching an automated apparatus built to reject frostbitten fruit by detecting dehydrated portions. In 1961, he built a prototype in which an X-ray source and a mechanically coupled detector rotated around the object to be imaged. By reconstructing the image, this instrument could get an X-ray picture of a nail surrounded by a circle of other nails, which made it impossible to X-ray from any single angle. In his landmark paper published in 1961, he described the basic concept which was later used by Allan McLeod Cormack to develop the mathematics behind computerized tomography.
In October 1963, Oldendorf received a U.S. patent for a "radiant energy apparatus for investigating selected areas of interior objects obscured by dense material." Oldendorf shared the 1975 Lasker award with Hounsfield for that discovery. The field of the mathematical methods of computerized tomography has seen a very active development since then, as is evident from overview literature by Frank Natterer and Gabor T. Herman, two of the pioneers in the this field.
Tomography has been one of the pillars of radiologic diagnostics until the late 1970s, when the availability of minicomputers and of the transverse axial scanning method gradually supplanted it as the modality of CT. Transverse axial scanning was due in large part to the work of Godfrey Hounsfield and South African-born Allan McLeod Cormack. In terms of mathematics, the method is based upon the use of the Radon Transform. But as Cormack remembered later, he had to find the solution himself since it was only in 1972 that he learned of the work of Radon, by chance.
Etymology
The word "tomography" is derived from the Greek tomos (slice) and graphein (to write). Computed tomography was originally known as the "EMI scan" as it was developed in the early 1970s at a research branch of EMI, a company best known today for its music and recording business. It was later known as computed axial tomography (CAT or CT scan) and body section röntgenography.
Although the term "computed tomography" could be used to describe positron emission tomography or single photon emission computed tomography (SPECT), in practice it usually refers to the computation of tomography from X-ray images, especially in older medical literature and smaller medical facilities.
In MeSH, "computed axial tomography" was used from 1977 to 1979, but the current indexing explicitly includes "X-ray" in the title.
Types of Machines
Spinning tube, commonly called spiral CT, or helical CT in which an entire X-ray tube is spun around the central axis of the area being scanned. These are the dominant type of scanners on the market because they have been manufactured longer and offer lower cost of production and purchase. The main limitation of this type is the bulk and inertia of the equipment (X-ray tube assembly and detector array on the opposite side of the circle) which limits the speed at which the equipment can spin. Some designs use two X-ray sources and detector arrays offset by an angle, as technique to improve temporal resolution.
Electron beam tomography (EBT) is a specific form of CT in which a large enough X-ray tube is constructed so that only the path of the electrons, travelling between the cathode and anode of the X-ray tube, are spun using deflection coils. This type had a major advantage since sweep speeds can be much faster, allowing for less blurry imaging of moving structures, such as the heart and arteries. Fewer scanners of this design have been produced when compared with spinning tube types, mainly due to the higher cost associated with building a much larger X-ray tube and detector array and limited anatomical coverage. Only one manufacturer (Imatron, later acquired by General electric) ever produced scanners of this design. Production ceased in early 2006.
See the whole article:
X-ray Computed Tomography From Wikipedia, the free encyclopedia.
No comments:
Post a Comment