Robotic Rehabilitation, Medical technology Volketswil, Switzerland
Hocoma is a privately hold globally active medical technology company based near Zurich, Switzerland. Hocoma was founded in 2000 as spin-off of the Spinal Cord Injury Center of the Balgrist University Hospital in Zurich, by the electrical and biomedical engineers Gery Colombo and Matthias Jörg and the economist Peter Hostettler. Today, Hocoma employs more than 110 people at its headquarter near Zurich and in its subsidiaries in Norwell, Massachusetts and Singapore. It develops therapy solutions for neurorehabilitation and low back pain therapy working closely with clinics and research centers. The Hocoma therapy solutions support the treatment of neurological patients with movement disorders caused by stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, cerebral palsy or other neurological diseases and injuries as well as low back pain patients.
Lokomat
The Lokomat is a gait therapy device on a treadmill with a robotic gait orthosis, and exercises in a virtual reality environment with a constant audio and visual feedback. The Lokomat also provides a pediatric orthosis for driven locomotion therapy for small children. The enhanced efficiency and efficacy of locomotion training with the Lokomat has been scientifically proven in over 100 publications in peer reviewed journals. That is more than any other robotic therapy device for lower extremity rehabilitation.
In 2011, U.S. News & World Report surveyed almost 5000 hospitals in the US and ranked them in 16 specialties. Nine out of ten hospitals ranked as the top ten in “Rehabilitation” offer gait therapy with Hocoma’s Lokomat. By the end of 2011, over 390 Lokomat devices were in clinical usages in hospitals and clinics worldwide.
Other products: Armeo Therapy Concept, Erigo, and Valedo.
See the full article Hocoma From Wikipedia, the free encyclopedia.
The Lokomat is the device that started Jeff's new journey. At the Rehabilitation Institute of Chicago, he was harnessed to the ceiling and lowered into the device with his son, Zack, looking on. Produced by Swiss robotic rehabilitation firm Hocoma, the machine is meant for "neurological patients with movement disorders caused by stroke, spinal cord injury, traumatic brain injury, multiple sclerosis or Parkinson's disease," according to the company. It was released in 2001.
Janet, 32 from Staffordshire who lives with her husband Karl, was participating in an Earls Court Exhibition when she suffered a stroke (intracerebral heamorrhage - ICH).
After major surgery Janet was admitted to the Acute Neurological Rehabilitation Unit at The Wellington Hospital. She was tiring very easily, her balance was very poor, she felt very dizzy and her speech was slurred. As a consequence she was unable to walk unaided and was dependent on help from the nursing staff for washing and dressing.
With the help of the team at the unit Janet set some goals on admission, which said that by discharge she would be able to get herself up and ready in the morning with a little help from her husband. (This included showering and dressing herself and applying her own make up and pinning up her hair).
Janet's rehabilitation programme consisted of Physiotherapy, Nursing, Occupational Therapy, Speech and Language Therapy and Neuropsychology, plus the use of some our latest technology including the Lokomat robotic walking device.
After 3 weeks, Janet was ready to return to Staffordshire to continue her rehabilitation nearer home. Janet had achieved her goal and was beginning to walk with assistance from her husband and was even able to wash her own hair, a huge achievement for her.
Madonna clinicians are currently undergoing intensive training sessions on the use of this cutting-edge piece of robotic equipment, which can help some people improve their ability to walk after disability caused by brain and spinal cord injuries, stroke, or neurological and orthopaedic conditions. Though the Lokomat is an effective and advanced rehabilitation tool, robot-assisted walking therapy is specialized and some medical conditions may limit its appropriateness for all people.
Studies show that locomotion therapy supported by a robotic assisted device on a treadmill is an effective intervention for improving over-ground walking function for those limited by illness or injury. The Lokomats specialized support and limb guidance, and the repetitive walking pattern, help the brain and spinal cord work together to re-route neural pathways, retraining the brain and body to facilitate the gait movements needed for walking.
In addition, Lokomat therapy helps strengthen muscles and improve cardiovascular health. The weight bearing aspect of the Lokomat may aid in the prevention of osteoporosis, building bone mass as the person assumes some of his or her own weight during therapy.
Madonna hopes to begin receiving patient referrals from physicians for the Lokomat in early 2010.
ARMY.MIL - After the crash of his helicopter, Crew Chief Spc. Mark Lalli is learning to walk again with the aid of an advanced set of robotic legs, a team of doctors, nurses, specialists, and...his mother. http://www.army.mil/news/health
Charles Remsberg, CEO of Hocoma Inc., demonstrates the Lokomat, the first driven gait orthosis that assists walking movements of gait-impaired patients. The Lokomat is used to improve mobility in individuals following stroke, spinal cord injury, traumatic brain injury, multiple sclerosis or other neurological diseases and injuries. For more information on this, and to see other interviews from CSM, visit http://www.therapytimes.com.
Lokomat Therapy, Armeo Therapy, Hyperbaric Oxygen Therapy, Therapy for Stroke, Therapy for SCI, Therapy for Multiple Sclerosis, Therapy for Cerebral Palsy.
Advanced Rehabilitation Equipment and Therapies for treating MS, Stroke, Spinal Cord and Traumatic Brain Injuries in Toronto, Canada please visit us at www.theraputix.ca Lokomat Therapy, Armeo Therapy, Hyperbaric Oxygen Therapy
May 31, 2012 — Scientists in Switzerland have developed a method to help paralyzed rats with severed spinal cords walk — and even climb stairs — again. The team's cocktail of neuron-activating chemicals and electrical stimulation might be a precursor to future treatments for disabled humans, researchers say.
Gabe goes to Theraputix for special therapy on the Locomat machine. Using complex support machinery and biofeedback he is walking his way back to independence.
For Better and For Worse Lynn Johnston - 2008-01-23 "His doctor thinks it's depression that ..."
Dilbert Scott Adams - 2013-04-22 "My invention will change the world ..."
Garfield Jim Davis -2013-04-24 "I've almost got you, cat !!"
Betty Delainey & Rasmussen - 2013-04-23 "I use the appropriate restroom ...."
*For Better and For Worse" is a serious topic of stroke but with a very nice cartoons. It is all about Grandpa Jim had a stroke and 88 further cartoon "strips" that happened to Grandpa Jim. (See as well the author Lynn Johnston).
** I tried to get low or free price at the people http://www.UniversalUclick.com/ for the images for the cartoons. It was too high for Stroke Survivors Tattler i.e. we are not a regular newspaper and our budget is very low. Fortunately, you will have to do only 1-click more to see the cartoon image, it is legit and it is free using GoComics.com and Dilbert.com.
*** Changed from "Pickles" to "Betty" -- "Betty" is a excellent cartoon and Gary Delainey & Gerry Rasmussen are authors/artists/cartoon-strips and they live in Edmonton.
I remember the doctor I got to prescribe me Lokomat training did not really believe in it, but I thought it was great. Motor Modules in Robot-Aided Walking.
Abstract (provisional)
Background
It is hypothesized that locomotion is achieved by means of rhythm generating networks (central pattern generators) and muscle activation generating networks. This modular organization can be partly identified from the analysis of the muscular activity by means of factorization algorithms. The activity of rhythm generating networks is described by activation signals whilst the muscle intervention generating network is represented by motor modules (muscle synergies). In this study, we extend the analysis of modular organization of walking to the case of robot-aided locomotion, at varying speed and body weight support level.
Methods
Non Negative Matrix Factorization was applied on surface electromyographic signals of 8 lower limb muscles of healthy subjects walking in gait robotic trainer at different walking velocities (1 to 3km/h) and levels of body weight support (0 to 30%).
Results
The muscular activity of volunteers could be described by low dimensionality (4 modules), as for overground walking. Moreover, the activation signals during robot-aided walking were bursts of activation timed at specific phases of the gait cycle, underlying an impulsive controller, as also observed in overground walking. This modular organization was consistent across the investigated speeds, body weight support level, and subjects.
Conclusions
These results indicate that walking in a Lokomat robotic trainer is achieved by similar motor modules and activation signals as overground walking and thus supports the use of robotic training for re-establishing natural walking patterns.
The complete article is available as a provisional PDF. The fully formatted PDF and HTML versions are in production.
Virtually every patient who comes to inpatient rehabilitation arrives with the goal to walk again, whether the patient's condition is due to a stroke, spinal cord or traumatic brain injury or other neurological issues.
My job as an inpatient rehab manager at Sheltering Arms Hospital in Richmond, VA, is to facilitate my team's ability to help patients realize this important but often difficult goal. Since I am also a clinician, I understand how challenging it can be to learn to walk again and also how crucial this skill is to quality of life.
Recently, I worked with a patient who had not walked in several weeks. She had a long hospital course with several surgical procedures, resulting in pain and dysfunction. When I asked this patient what her goals for physical therapy were, her answer was simple but familiar: "I just want to walk."
Although she was severely debilitated, I was determined to help her attain her goal. A rehab technician and I attempted to help her stand with a walker and move her legs, but after only a few steps we were all totally exhausted. If you are a PT in inpatient rehabilitation, this frustrating situation is probably one you know well.
Principles of motor learning and neuroplasticity tell us that repetition is essential for recovery. Yet how can a patient possibly learn and recover if he or she is only able to walk a few steps at a time? How can physical therapists help patients meet the goal to resume walking and recover faster using evidence-based practice?
The Role of a Rehab Manager
Although most of us take it for granted, the ability to walk independently is required for most daily activities. The majority of patients need to be able to walk fast enough to function in the community in order to return to prior level of mobility.
The unfortunate fact is that studies have shown only 7 percent of patients discharged from rehabilitation meet the criteria for community walking, which includes the ability to cross a road safely, and they continue to demonstrate gait patterns that deviate from the norm. This tells the therapy community that we, as caregivers and rehabilitation experts, could do better.
Part of my responsibility as an inpatient rehab manager is providing the finest tools and resources that enable therapists to deliver the best possible care to each patient. Yet there are hundreds of different devices on the market, and it can be difficult to determine which technology is the best fit for a clinic or specific patient populations.
Any new technology must be appropriate for the patient and be designed based on the most recent evidence in motor learning. The technology must also be easy to use; if a piece of equipment takes too long to set up or is difficult to operate, therapists simply will not use it. They want to use their time-and the patient's time-wisely.
Stepping Forward with Technology
At Sheltering Arms we are fortunate to have the resources to acquire new technologies to supplement physical therapy expertise. Our iWALK Recovery Center program includes inpatient and outpatient services built upon the latest research in assessment and intervention.
The center was created to provide the most advanced technologies available to help patients walk again. Our goal is to have a variety of equipment and technology to meet the needs of patients with a range of diagnoses and functional abilities, all in one place. Patients who have reached a plateau with other therapies or who have been living with debilitating conditions for years finally have a resource to make progress.
The iWALK therapy team is also trained in neurorecovery-without highly trained experts to effectively use and operate the technology, devices and equipment cannot deliver on their promise.
After all, these are just tools; without the clinical judgment and expertise of a therapist, they would be useless. The therapist determines the right tool for the right patient at the right time.
Choosing Your Tools
New technologies are designed based on principles of motor learning and the relatively new concept of neuroplasticity; it has not always been known that the brain is capable of modification after injury.
In the case of my patient mentioned above, this is the point where technology came into play for her rehabilitation. After the frustrating effort to help her take a few steps with a walker, we fit her with a harness and hooked it into a dynamic over-ground body weight support system.
Lokomat is a Gait Therapy Device
The system took some of her body weight away and she was able to stand. Instantly, she was able to move more freely and, with a walker and tactile cues, this patient was able to walk 50 feet over ground. Her relief was clear; she realized that her goals were within reach. She would walk again.
The over-ground body weight support system is just one example of technology that can be used to capitalize on the theories of neurorecovery while keeping patients safe and engaged in therapy.
Because it is a dynamic system and can be used over ground or over a treadmill, patients experience walking in a real-world environment and are safe from falling. Patients are even able to experience loss of balance by being able to fall up to six inches before the system "catches" them.
As recent research indicates, it is important for patients to experience error in order to promote learning in the neural pathways. Coupled with a split-belt treadmill, which uses the principle of motor adaptation to improve asymmetric gait patterns, many patients are able to recover much faster than previously possible.
In addition, advances in functional electrical stimulation (FES) have resulted in the ability to cue and facilitate muscle activity during functional activities. For example, we frequently use a cuff that fits on the patient's lower leg and has three components that communicate with each other through wireless technology to stimulate the muscles used to lift the foot while walking. It is especially useful because it allows for real-time adjustments and adaptations according to the patient's gait pattern.
Recently, we started using a new expansion on the technology that was cleared by the FDA earlier this year. This includes a thigh cuff that works along with the lower leg cuff to stimulate the quad or hamstring muscles used during walking and allows for even greater facilitation of gait kinematics.
Although the technology was just commercially released and is new in our facility, patients are already seeing results from working with the new thigh cuff. Our therapists use these technologies frequently because they are easy to use and can be set up in less than 15 minutes and patients are motivated and engaged by their use.
While the ultimate resource is the expertise and judgment of the therapist, these kinds of advances in the rehabilitation tool kit enable patients to practice walking with appropriate kinematics earlier in their rehabilitation course and promote recovery of the central nervous system.
Early rehabilitation has been associated with improved functional outcomes and quality of life following a stroke. Therapists need to have the right tools and expertise to help patients improve more quickly and ultimately attain a higher level of recovery.
At Sheltering Arms, our patients benefit from our ability to provide walking retraining earlier in their recovery process. When considering how to best approach patients hoping to walk again, it is important to consider the exciting advances in our constantly evolving field, and how to best marry technological power with clinical expertise.
Before even doing anything an objective assessment like this would be good.
I've been trying to get Bob's peg tube replaced since January. That's right. January.
This because I am being smart, or so I thought, by staying ahead of the game. Nipping a problem in the bud, before it blooms. Because I know Bob's peg tube is on it's last legs. And would need to be replaced. About right now.
So back in January, I get a referral for a new GI doc from Bob's primary care doctor. Because I don't want to go back to the old GI doc. As he is pretty useless. Not to mention he works out of The Hospital. And we don't want to go back there. For obvious reasons.
In January, I called the new GI doc's office to set up an appointment and am told immediately that they don't take Bob's insurance. Which is weird. Because they are on the insurance company's website. At least I think. So I hang up the phone and go on the insurance company's website and sure enough, they are listed as a provider. So I call the office back up and the receptionist, first, argues with me that my information is wrong. Then finally connects me to someone else, who tells me they do in fact take his insurance. I ask if I can set up an appointment, please. But she wants to know what the purpose of this appointment would be. So I tell her that my husband has a peg tube and it will need to be replaced soon. Then she tells me that this particular GI doctor will not work on a peg tube that he did not put in and I need to go back to the GI doctor who put the peg tube in.
Huh?
So after another argument, finally, she tells me to have all of Bob's medical records transferred over to their office at which time the GI doc will review them and decide if he wants to take Bob as a patient. And if he decides it's OK, they will contact me for an appointment.
Okey dokey. Though I'm thinking this is really weird. I didn't know that doctors could "pick and choose" which patients they wanted to see.
But I do this, call to have all the records transferred over. And I wait. And I don't hear from them. So, in February, I call the GI doctor's office again, this time I just schedule an appointment. I figure if the doctor doesn't want to see us, well, he can throw us out of the office when we get there.
We went to see the new GI doctor on March 4th. I tell him that Bob's peg tube will need to be replaced soon and I'd like to get it done now, before it starts causing all sorts of problems and the whole thing turns into an emergency. Think: Kaboom! Like his first peg tube did when it burst and split down the side...
The doc looks at Bob's peg tube and agrees that it probably only has a month of life left in it. Then he tells me that Bob will need to stop taking his warfarin five days before the procedure. And I tell him that he cannot go off the warfarin because he has hyper-coagulating blood and is a high stroke risk. And that this is Bob's third tube and both times it was replaced before, the procedure was done while on warfarin. And he tells me that this is too risky and the other doctors were wrong to do the procedure while on the warfarin. We go round for round on this for a bit, then the doctor says he could switch Bob from warfarin to lovenox which is a fast-acting blood thinner, then stop of the lovenox for a "small window of time" during the procedure, then put him back on the warfarin, but he will have to talk to Bob's neuro doctor and discuss how to do this first.
We leave the doctor's office with the promise that once he talks with the neuro doc someone will call me and set up an appointment for Bob's peg tube replacement. And also, he will order a home health nurse to come to our house to administer the lovenox. Which is an injection.
All righty.
Once again I wait. Two weeks pass and no one calls me. So I call the GI doctor's office and after leaving a billion messages, finally, a week later, the nurse calls me back and tells me they are still waiting for a response from the neuro doc to the fax that they sent. So, I call the neuro doc and talk to his assistant who tells me they never received a fax. So I call the GI doctor's office back and leave another billion messages and finally, a week later, the nurse returns my calls and says she will re-fax the request.
Oh-kay....
And I wait. Again. And no one contacts me.
Meanwhile, Bob's peg tube is getting wonky. That's a technical medical term. Wonky. Meaning, it's clogging every darn morning. It's ballooning up. It's kinking. It doesn't look good.
Now add this to my ever-growing resume: Master of the Clogged Peg Tube. Because after two plus years, I have become an expert on this matter. And you can forget about using Coca Cola, or Adolf's Meat Tenderizer or Hot Coffee or all the other strange old wives tales out there, because the best and fail-safe way to unclog a peg tube is with warm tap water and a cannula brush. First, you run the brush through the tube like a roto-rooter, then flush with warm tap water. This never fails.
Until yesterday....
But I am jumping ahead of myself. Because before yesterday, I once again called the GI doc's office and left two billion more messages and finally, a week later, the nurse calls me back and tells me they are still waiting for a response from the neuro doctor... So I tell her that this is getting pretty ridiculous and Bob's tube is going, I mean, really going. And if it goes, we will end up over at ER and the reason I contacted their office way back in January was to prevent this from happening.... and she asks me if there is another doctor that could respond to their request, so I give her the name of Bob's primary care doctor. She says she will fax the neuro doc again and also fax a request to the primary care doctor.
All right.
And I wait. Again....
Earlier this week, I call the GI doctor's office and leave another billion messages for the nurse, who does not call me back. On Thursday, Bob had an appointment with his primary care doc. So I ask him, if he got a fax, and he did not. So I explain the whole problem and show him how wonky Bob's tube is getting and he tells me that he does not want to get involved with this and I need to make an appointment to see the neuro doc ASAP and discuss this matter with him. Then I tell him that I don't think this GI doctor knows what he's doing and can he refer us to someone else? And he tells me that I should not go hopping from one doctor to another!
Jeepers.
Well, I am not about to make an appointment to see the neuro doc because it will take weeks to get in, plus it will cost $35.00 plus the cost of wheelchair transport and I am not spending that kind of money to ask a doctor if he got a fax.
So we get home from the primary doc's office and I call the neuro doc's office and talk to the medical assistant again and she says they still have not gotten a fax from the GI doctor. So I call the GI doctor's office and, miraculously, the nurse answers the phone! I tell you, I nearly fell over dead. And she promises me, promises me that she will walk to the fax machine as soon as she hangs up the phone and fax another request.
That was Thursday.
Which brings me back to yesterday morning.
When for the life of me, I could not unclog Bob's peg tube. I mean, I spent forty-five freaking minutes trying to unclog that tube. Nothing was working. My cannula brush was hitting what seemed to be concrete. The wire end of the brush bending instead of going through. Then tube itself was rock hard in parts and the thing was ballooning, like a long sausage shaped water balloon. I was afraid it might burst. I tried warm water, then HOT water. And I pushed that syringe as hard as I could, and the darn water would burst out through the Y-port and drench both me and Bob. And still the tube was clogged. And I attempted to roto-rooter the tube every which way. I was to the point of meltdown. Furious. The kind of furious where you want to stamp your feet and throw things across the room and GAAAA! scream your head off. And of course I was furious at the doctor's office and the nurse who won't return calls and the faxes which disappear into a black hole. And then I just wanted to sit down in the middle of the floor and cry my eyes out. Because I would have to take Bob to ER if I didn't get the darn thing unclogged, then they would admit him to the hospital to wean him off warfarin, which could take like five freaking days. And oh lord. I needed to get creative here.
I knew the trick was to warm the tube up. So I got a bright idea. I got a big soup bowl out and filled it with hot water. I draped Bob with a big bath towel. Then I took that tube and coiled it like a snake and submerged it in the hot water. Thinking that I could warm it up from the outside. And it seemed to be working because the concrete blockage was no longer rock hard. The tube was growing flexible again. But the problem was that I couldn't get the whole tube into the soup bowl, I mean, especially the part that goes into Bob. So I got another bright idea. I took some wet towels and nuked them in the microwave and then wrapped Bob's tube in them and let it sit for a few minutes. After that, I massaged his tube with my fingers trying to break up the clog.
Then I took the cannula brush and whoo hoo! It went through! But when I tried to syringe water through the tube, all I got was that damnable long sausage shaped water balloon. And nothing else. Except water spewing back out of the Y-port all over me and Bob and the sofa next to Bob's bed.
grrrr....
I was desperate. When your desperate, you resort to desperate measures. So I got out the scissors and I syringed water into the tube until the big sausage shaped water balloon appeared. I pinched the place where the balloon started with my fingers, withdrew the water back into the syringe, then I snipped the tube, cut off the part of the tube where the sausage balloon had appeared, and it was a good six inches, I swear. But now I could see into the tube, see what was blocking it, and weirdly enough, there was nothing there. I ran the brush through Bob's now foreshortened tube, and it went through. So I reattached the Y-port and, lo and behold, was able to syringe in the water. Able to get his morning meds into him.
Easy as that.
That afternoon, I called the neuro doctor's office and talked with medical assistant again because I wanted to make sure she got the fax that was supposedly sent out yesterday. She said that she gotten it. Then she said that they had gotten this same fax three times before and had just filed it, thinking it was for "information purposes only".
GAAAA!
You can bet, I will be on the phone again next week. Because I can't keep chopping bits off Bob's tube or soon he'll have nothing left!
Things should not be this hard.
3 comments:
J.L. Murphey April 20, 2013 said... Diane, Do you have someone to sit with Bob for an hour or so? If so hand carry the request to the neuro and back to the GI. This is ridiculous! The electronic and phone tag needs to stop. You shouldn't have to do all of this. First off, doctors have the right to refuse any patient care when referred by another doctor to accept the patient. I know it sounds wrong but it is the truth. I've quit doctors and had doctors quit me and yes, even refuse to see me. The next time it gets clogged have him transported to the ER. I guarantee somebody will fix the problem especially when you tell them the stuff you've been going through since January. I know you hate going to the hospital because of the suit BUT the doctors are being unreasonable and you've got to have help. It's not like you have a choice of five or six different hospitals to choose from. We are in the same boat here. They have to care for us no matter what. Susan April 20, 2013 said... Holy Cow Diane, I was exhausted and furious at these doctors after I read your blog! I called Dahn's primary doctor last Wednesday, never got a call back, then I called last Friday, and I am still waiting for a call back!! The anxiety this causes is horrible and unecessary! Right now I am stomping my foot and letting out a scream....lol! Joyce April 22, 2013 said... Diane ! The run around you are getting is crap!!! I don't know what to tell you , but sounds like you are dealing with it and keeping your sanity too. I don't think I could do that and remain sane. I am so impressed with your resourcefulness in working with his tube. I feel so fortunate , as have not had any major problems with garys tube. His is a different kind though, as it snaps in place when I feed him and then come off so I can wash it. The first one he had was like Bobs.. I like this one much better. I wish you luck :) Joyce
The response from my aphasia blogs have garnered a lot of questions and responses so I thought to revisit this subject today and give you a progress report. Since I am no longer in speech therapy because of best use of my rehab visits, I started a seat-of-my-pants training schedule as you may have read about in previous posts.
In college, I learned for each hour of class time I needed to spend two hours in study time. With stroke deficits, the ratio is more like for every hour of professional time (with the therapist) spent I have to do six hours of study/ practice time. It boggles the mind doesn't it? Especially when you consider the fact that I spend six hours in professional therapy hours a week, it equates to thirty-six hours of at home practice. That's a huge chunk of time.
Is it necessary? It depends. How bad do you want to recover? For me, I want/need to recover all that I can. Do I have the stamina to continue this for the years it may take? I dunno. We'll have to see. I'm almost a year out from my stroke and have continued my therapy program adding new, fun ways to do it to keep it interesting.
James at Easter 2013
When I first struggled with forming words and creating sounds, I used my grandson. Yes, I said used because, being less than a year old, he was trying to form sounds and words also. We were in the same boat. He was learning and I was relearning. Not to mention he's cute and just loves his Oma (the German word for Grandmother). He would sit on my lap in the wheelchair mimicking me. It was fun to watch him as I did my exercises for hours on end. I'm still amazed by the attention span this baby, then a seven-month old, had.
I had to learn how to form the words right with my lips because my husband reads lips. He's deaf. The sounds wasn't necessary except for communicating with the outside world. But we have family which needs to be talked to so making myself understood was important also.
I often forget he can't hear in our conversations until he reminds me that my head was turned away. He'll say, "I can't hear you. Repeat that."
This is just one of my life's little challenges I have to overcome with aphasia. I find the more I practice the better I get. When we go to McDonalds, I'll stand at the counter and order. I remember what my speech therapist told me, "Slow, loud and clear." So I might stumble over my words and get weird looks from the cashier or waitress in a restaurant, who cares? I'm practicing and vocalizing. If I get too flustered I can always point in the menu or make the symbol for the number I'm ordering with my fingers. The point is that I'm making an effort. Not making an effort or letting someone else do the talking for me is easier, but what benefit is it to me and my recovery?
The words are coming easier now without the extremely long pauses in between. I'll still lose words and have to back track when speaking. Using inappropriate words for things- not so much as a few months ago. I'm constantly being corrected by those around me in a loving way. I can always count on my #2 and #4 daughters to correct with humor. My #4 daughter also suffers from a mild form of aphasia. In that case, it's the affected correcting the affected, and we'll poke fun at each other.
The real trick is when both of us can't remember a word. But there are usually others around to play twenty questions. Our oldest daughter will cock her hand at the wrist and hit her chest and go, "D-a-a-a-a-h!" in a totally stupid way. My husband will outstretch his arms in front of him, with palms out clapping, and barking like a seal. Either response brings laughter. Having this kind of loving support is essential to my recovering my speech.
While I have trouble speaking, I found it has been easier to find the words when I type. So increasing to amount I blog is working. At least it is getting easier as I go along. This is also my home therapy regime. I imagine my readers are tired of my constant blogs, but this I do for me. It helps with my strategy and planning deficits too. Having a plan makes it easier on my mind for focusing. This particular blog was written April 10th for example to give me time to find any errors. I read this blog aloud to my husband to practice my vocal and reading skills. It's a relearning triangle that goes full circle. It's how we learned these skills in the first place.
I noticed I have my kitty speaking voice intonations back. When that happened, I dunno. What is a kitty speaking voice? It's that cute, cuddly voice I use towards my cats and young grandchildren. Like what you would use when confronted with the kitten to the right and how would you say it? The higher pitched, sing songy voice we all have and use. So I'm not quite strictly monotone anymore. Yeah me!
I still have not managed humor or sarcasm yet, but I'm confident I'll get those back too.
The cognitive difficulties, I'll address in another post.
Nothing is impossible with determination!
4 comments: Lara April 21, 2013 said... Glad you're doing better, Jo! I do have a question, if it's not too bold of me to ask: did you find that your aphasia extended to your writing, or only your speaking? Hilary Melton-Butcher April 22, 2013 said... Hi JL - thanks for updating us and letting us know you used your grandson - he must have had so much fun! Then your husband being deaf ... The strokes my mother had gave her left-sided neglect, slightly gave her a speech impediment which came and went .. but things improved dramatically - and in your case I'm sure will continue. Great that you're reading the posts to your husband, and getting that feedback ... My mother lost her hearing at one stage - and it was so funny .. not really for her, as she didn't know she'd lost her hearing .. so she could talk, but made up what I said ... a real life tv drama at times. I laughed my way through - she couldn't read properly - words were ok .. but not sentences. She was in hospital for a while .. I found her one day muttering D words to herself .. she said she was remembering as many D words as possible - so her brain didn't stultify ... it didn't. We had some incredible times .. and I really wouldn't have wanted her to be stroked, but those last 5+ years had some great laughs and learning curves ... Thanks for keeping on writing .. I'll pay more attention in future .. Cheers and with thoughts - Hilary J.L. Murphey April 22, 2013 said... Lara, With my writing it's a cognitive deficit. While I used to hate the spelling and grammar checkers, I can't write without them now. There isn't a sentence I type that doesn't have red and green squiggly lines in it. There is also the word loss. I compensate by filling a description of the word in parentheses and have to go back and fill the word in. So it's slow going but I am at least writing. So many stroke survivors have lost their ability to read, write, and even form sentences. I'm lucky. J.L. Murphey April 22, 2013 said... Hilary, I work hard not to have right sided neglect. I purposefully try to use my right arm as much as possible like turning on a light switch. Granted it takes using the whole arm to do it, but I'm preventing the neglect. Factors like energy level, stress, and drugs all affect my ability to speak and finding words. A stroke survivor friend of mine only remembered how to say "shut up" and another it was "love you." It's funny want the brain remembers. Hilary, I'm here almost everyday. Thanks for popping in and commenting.
With the lower extremity "function" is inherently bilateral. That is, because the primary function of the lower extremities is ambulation, bilaterality is inherent.
(By "advantage" I do not suggest that I buy into the concept that the lower extremities come back before the upper extremities post-stroke. This is common wisdom in rehab, but it may be incorrect. The only way to prove the lower extremity comes back before the upper extremity would be to measure the most distal element of both: the fingers and toes. Measuring toe extension in comparison to finger extension has, to my knowledge, never been done.)
Beyond bilaterality, ambulation is also inherently rhythmic. The rhythm after stroke is disrupted and made unequal. And rhythm is what bilateral leg training with rhythmic auditory cueing attempts to re-establish in the lower extremity.
That is, if you re-establish the rhythm of gait, you will go a long way to re-establish symmetry of both step length and step timing.
There are commercial systems that use a heel switch so that the moment of heel strike is radio-delivered to headphones. The patient hears their own heel strike through the headphones, as well as a beat that they have to match with each heel strike.
But as is true with many technologies purported to help stroke survivors relearn movement, no special system is really needed to bring the idea of rhythmicity into gait.
A simple metronome either heard through headphones or carried by the therapist next to the stroke survivor can be used to promote the re-establishment of rhythmicity of gait. Plugging the ears using standard noise-reducing plugs can boost the volume of footfall to make that obvious to the survivor. The trick is then to match the footfall to the beat.
1 comment:
The Liberal Capitalist April 17, 2013 said... In inpatient and later outpatient rehab, my PTs did an excellent job of helping me attain a nice, rhythmic gait. I spent what seemed like endless hours on a treadmill gait-trainer and marching around the hallways connected to my PT by gait poles. When I came home, I enjoyed walking around our neighborhood for up to an hour at a time. That changed when spasticity attacked at around nine months post. Now at 18 months post, it has gradually gotten worse. I still walk, but it isn't nearly as enjoyable, or easy. I have to choose the stride for my affected leg, either straight, unbent knee, or a folding-knife-blade snap. I concentrate on trying to achieve a normal gait, and that pretty much takes the fun out of walking. Oh well, as my wife points out, I can walk, and that's al lot to be thankful for.
Doing 80 repetitions while wearing the Releas splint made my hand tighter. I don't know if this would have happened if I hadn't stopped using the SaeboFlex splint for five months after I broke my forearm. SaeboFlex exercises reduce the flexor tone in my hand for 24 hours. Now I use the Releas splint to help me during ADLs with thin objects, like inserting a return slip and check in an envelope. After I close my hand on an envelope the Releas splint helps me let go. My hand was completely flaccid for three months so the photo on the right feels like a small miracle.
Folding laundry one-handed is aggravating and takes forever. As I straighten one section of a garment I drag another section out of place. The photo on the left shows my hands just before I lift my right hemiplegic thumb so my sound hand can put the two halves of the fabric together. When the two halves touch I press down with my hemiplegic thumb to hold them together. The problem is once I pinch it is hard to let go without help from the Releas.
Wearing the Releas splint during functional activities changed the way I do SaeboFlex exercises. I pick up a ball, transfer it to my hemiplegic hand, and set the ball on the table. To keep the ball from rolling off the table I place the ball in a glass custard cup. Then my hemiplegic hand pick ups the ball and drop it in a crate. I hope to graduate to an inverted peanut butter jar lid and then a towel as my ability to open my hand at arms length improves.
A stroke taught me my non-dominant hand needs to reach for objects on counters and hold them still. The photo on the right is a sample of objects that require this skill able-bodied people take for granted. The Releas splint taught me I need to stop thinking of exercise when I use the SaeboFlex splint. I put out a bottle of soy sauce to help me remember the goal the SaeboFlex splint is preparing me for.
3 comments:
J.L. Murphey April 14, 2013 said... WTG on multi tasking your splints. oc1dean April 17, 2013 said... Until I get my wrist spasticity to stop, holding things upright on the counter is an exercise in tipping things over. But this might get me back to therapy. Rebecca Dutton April 20, 2013 said... An unexpected consequence of doing so many exercises where I turn my palm up and down is that my wrist is more relaxed. Probably not enough for someone to see a difference, but enough for me to feel less resistance at the end of wrist movement.
It's the first "Anderson's Viewers Got Talent"! On Monday's show, Sharon Osbourne and Carrie Ann Inaba -- from two of the most popular competition shows on TV -- join forces to help Anderson judge.
D. Westry, an artist from Georgia, takes the stage and creates an amazing portrait of Anderson in just two minutes. After judges Anderson, Carrie Ann Inaba and Sharon Osbourne realize what the painting is, Anderson says, "I thought it was a weird potato!"
January 2013
Here is something a bit random, but nonetheless astounding. A work mate of mine who is also a photographer captured what is, to me, one of the most remarkable things I have ever seen filmed.
It is a 3 minute video clip of the full moon rising over Wellington. It was shot 2 nights ago, on a calm summer evening, as people gathered on the Mt. Victoria Lookout point to watch the moon rise.
This stunning video is one single real-time shot, with no manipulation whatsoever. The camera was placed on a hillside over 2 kilometres from the Lookout point, and was shot with the equivalent of a 1300mm lens.
The amount of planning, trial and error, and luck that went into this are mind blowing. He has been trying to capture this for over a year with many failed attempts. But 2 nights ago it seems everything was on his side, and it all came together in a way even he couldn't have hoped.
I honestly can't say enough good things about this video - from the magnitude of the visuals, to the intimate stories playing out with the people, to the sheer humbling nature of seeing the awe-inspiring reality of this giant rock in the sky that we so often don't stop to appreciate.
One thing I encourage you to do is watch this on the biggest screen you have - don't waste it on an iPhone screen. May it leave you breathless in the face of such majesty. Better than any church service you could ever attend.
Full Moon Silhouettes
Full Moon Silhouettes is a real time video of the moon rising over the Mount Victoria Lookout in Wellington, New Zealand. People had gathered up there this night to get the best view possible of the moon rising. I captured the video from 2.1km away on the other side of the city. It's something that I've been wanting to photograph for a long time now, and a lot of planning and failed attempts had taken place. Finally, during moon rise on the 28th January 2013, everything fell into place and I got my footage.
The video is as it came off the memory card and there has been no manipulation whatsoever. Technically it was quite a challenge to get the final result. I shot it on a Canon ID MkIV in video mode with a Canon EF 500mm f/4L and a Canon 2x extender II, giving me the equivalent focal length of 1300mm.
Until now, the last article for the week on SSTattler is some article I picked in Edmonton that will tell you about the new symphony or rock music festival or car show or various local events that will be nice for Stroke Survivors. I tried to minimize for the cost and some events was often free. But... it was very few people went to the events; I tried to find an alternative but I'm stumped - until now!
Published on Jan 23, 2013 SSTattler: Malanka - I'm a little late but you have to see it and go to it next year!
Rick visits Saskatoon, SK where he learns Ukrainian dance steps to help celebrate Malanka -- the new year according to the Julian calendar.
Comments 94 and going up! Богдан Паламарчук: Вауууу дуже сподобався сюжет. (Я живу в Україні) Translate by Google: Wowwwww really liked the plot. (I live in Ukraine) Jessica-Robyn W.: I did not know that we had so many Ukrainian's in Canada! Their celebrations look fantastic! Wow :D Роман Чернига: В україні меньше святкують ніж там :) Translate by Google: In Ukraine less celebrated than there :) See the 94+ full comments inRMR: Ukrainian New Year in YouTube
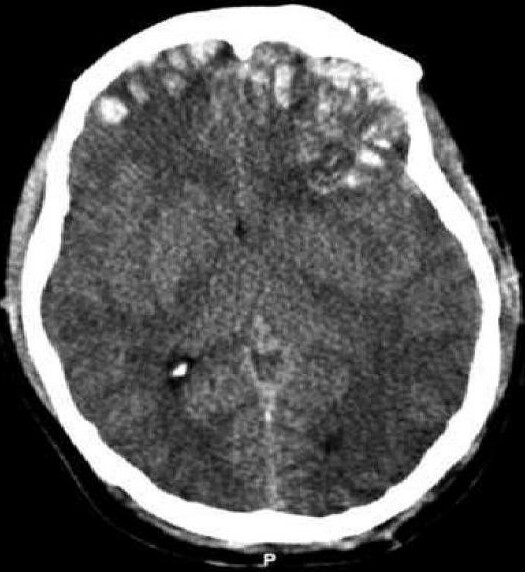
Traumatic Brain Injury
Classification and external resources:
CT scan showing cerebral contusions,
hemorrhage within the hemispheres,
subdural hematoma, and skull fractures. SSTattler: Strokes can be classified into two major categories: ischemic and hemorrhagic; Traumatic Brain Injury (TBI) occurs when an external force traumatically injures the brain. Both, stroke and TBI, have similar results and need for physical therapy, speech therapy, recreation therapy, occupational therapy, vision therapy,... Note: This is a LONG article and so SSTattler we will present a sub-set -- see the full article for more of information for TBI.
Traumatic brain injury (TBI), also known as intracranial injury, occurs when an external force traumatically injures the brain. TBI can be classified based on severity, mechanism (closed or penetrating head injury), or other features (e.g., occurring in a specific location or over a widespread area). Head injury usually refers to TBI, but is a broader category because it can involve damage to structures other than the brain, such as the scalp and skull.
TBI is a major cause of death and disability worldwide, especially in children and young adults. Males sustain traumatic brain injuries more frequently than do females. Causes include falls, vehicle accidents, and violence. Prevention measures include use of technology to protect those suffering from automobile accidents, such as seat belts and sports or motorcycle helmets, as well as efforts to reduce the number of automobile accidents, such as safety education programs and enforcement of traffic laws.
Brain trauma can be caused by a direct impact or by acceleration alone. In addition to the damage caused at the moment of injury, brain trauma causes secondary injury, a variety of events that take place in the minutes and days following the injury. These processes, which include alterations in cerebral blood flow and the pressure within the skull, contribute substantially to the damage from the initial injury.
TBI can cause a host of physical, cognitive, social, emotional, and behavioural effects, and outcome can range from complete recovery to permanent disability or death. The 20th century saw critical developments in diagnosis and treatment that decreased death rates and improved outcome. Some of the current imaging techniques used for diagnosis and treatment include CT scans computed tomography and MRIs magnetic resonance imaging. Depending on the injury, treatment required may be minimal or may include interventions such as medications, emergency surgery or surgery years later. Physical therapy, speech therapy, recreation therapy, occupational therapy and vision therapy may be employed for rehabilitation.
Classification
Traumatic brain injury is defined as damage to the brain resulting from external mechanical force, such as rapid acceleration or deceleration, impact, blast waves, or penetration by a projectile. Brain function is temporarily or permanently impaired and structural damage may or may not be detectable with current technology.
TBI is one of two subsets of acquired brain injury (brain damage that occur after birth); the other subset is non-traumatic brain injury, which does not involve external mechanical force (examples include stroke and infection). All traumatic brain injuries are head injuries, but the latter term may also refer to injury to other parts of the head. However, the terms head injury and brain injury are often used interchangeably. Similarly, brain injuries fall under the classification of central nervous system injuries and neurotrauma. In neuropsychology research literature, in general the term "traumatic brain injury" is used to refer to non-penetrating traumatic brain injuries.
TBI is usually classified based on severity, anatomical features of the injury, and the mechanism (the causative forces). Mechanism-related classification divides TBI into closed and penetrating head injury. A closed (also called nonpenetrating, or blunt) injury occurs when the brain is not exposed. A penetrating, or open, head injury occurs when an object pierces the skull and breaches the dura mater, the outermost membrane surrounding the brain.
Pathological Features
CT scan Spread of the:
subdural hematoma (single arrows),
midline shift (double arrows)
Systems also exist to classify TBI by its pathological features. Lesions can be extra-axial, (occurring within the skull but outside of the brain) or intra-axial (occurring within the brain tissue). Damage from TBI can be focal or diffuse, confined to specific areas or distributed in a more general manner, respectively. However, it is common for both types of injury to exist in a given case.
Diffuse injury manifests with little apparent damage in neuroimaging studies, but lesions can be seen with microscopy techniques post-mortem, and in the early 2000s, researchers discovered that diffusion tensor imaging (DTI), a way of processing MRI images that shows white matter tracts, was an effective tool for displaying the extent of diffuse axonal injury. Types of injuries considered diffuse include edema (swelling) and diffuse axonal injury, which is widespread damage to axons including white matter tracts and projections to the cortex. Types of injuries considered diffuse include concussion and diffuse axonal injury, widespread damage to axons in areas including white matter and the cerebral hemispheres.
Focal injuries often produce symptoms related to the functions of the damaged area. Research shows that the most common areas to have focal lesions in non-penetrating traumatic brain injury are the orbitofrontal cortex (the lower surface of the frontal lobes) and the anterior temporal lobes, areas that are involved in social behavior, emotion regulation, olfaction, and decision-making, hence the common social/emotional and judgment deficits following moderate-severe TBI. Symptoms such as hemiparesis or aphasia can also occur when less commonly affected areas such as motor or language areas are, respectively, damaged.
One type of focal injury, cerebral laceration, occurs when the tissue is cut or torn. Such tearing is common in orbitofrontal cortex in particular, because of bony protrusions on the interior skull ridge above the eyes. In a similar injury, cerebral contusion (bruising of brain tissue), blood is mixed among tissue. In contrast, intracranial hemorrhage involves bleeding that is not mixed with tissue.
Hematomas, also focal lesions, are collections of blood in or around the brain that can result from hemorrhage. Intracerebral hemorrhage, with bleeding in the brain tissue itself, is an intra-axial lesion. Extra-axial lesions include epidural hematoma, subdural hematoma, subarachnoid hemorrhage, and intraventricular hemorrhage. Epidural hematoma involves bleeding into the area between the skull and the dura mater, the outermost of the three membranes surrounding the brain. In subdural hematoma, bleeding occurs between the dura and the arachnoid mater. Subarachnoid hemorrhage involves bleeding into the space between the arachnoid membrane and the pia mater. Intraventricular hemorrhage occurs when there is bleeding in the ventricles.
Signs and Symptoms
Unequal pupil size is potentially a sign of a serious brain injury
Symptoms are dependent on the type of TBI (diffuse or focal) and the part of the brain that is affected. Unconsciousness tends to last longer for people with injuries on the left side of the brain than for those with injuries on the right. Symptoms are also dependent on the injury's severity. With mild TBI, the patient may remain conscious or may lose consciousness for a few seconds or minutes. Other symptoms of mild TBI include headache, vomiting, nausea, lack of motor coordination, dizziness, difficulty balancing, lightheadedness, blurred vision or tired eyes, ringing in the ears, bad taste in the mouth, fatigue or lethargy, and changes in sleep patterns. Cognitive and emotional symptoms include behavioral or mood changes, confusion, and trouble with memory, concentration, attention, or thinking. Mild TBI symptoms may also be present in moderate and severe injuries.
A person with a moderate or severe TBI may have a headache that does not go away, repeated vomiting or nausea, convulsions, an inability to awaken, dilation of one or both pupils, slurred speech, aphasia (word-finding difficulties), dysarthria (muscle weakness that causes disordered speech), weakness or numbness in the limbs, loss of coordination, confusion, restlessness, or agitation. Common long-term symptoms of moderate to severe TBI are changes in appropriate social behavior, deficits in social judgment, and cognitive changes, especially problems with sustained attention, processing speed, and executive functioning. Alexithymia, a deficiency in identifying, understanding, processing, and describing emotions occurs in 60.9% of individuals with TBI.[40] Cognitive and social deficits have long-term consequences for the daily lives of people with moderate to severe TBI, but can be improved with appropriate rehabilitation.
When the pressure within the skull (intracranial pressure, abbreviated ICP) rises too high, it can be deadly. Signs of increased ICP include decreasing level of consciousness, paralysis or weakness on one side of the body, and a blown pupil, one that fails to constrict in response to light or is slow to do so. Cushing's triad, a slow heart rate with high blood pressure and respiratory depression is a classic manifestation of significantly raised ICP. Anisocoria, unequal pupil size, is another sign of serious TBI. Abnormal posturing, a characteristic positioning of the limbs caused by severe diffuse injury or high ICP, is an ominous sign.
Small children with moderate to severe TBI may have some of these symptoms but have difficulty communicating them. Other signs seen in young children include persistent crying, inability to be consoled, listlessness, refusal to nurse or eat, and irritability.
Causes
The most common causes of TBI in the U.S. include violence, transportation accidents, construction, and sports. Motor bikes are major causes, increasing in significance in developing countries as other causes reduce. The estimates that between 1.6 and 3.8 million traumatic brain injuries each year are a result of sports and recreation activities in the US. In children aged two to four, falls are the most common cause of TBI, while in older children traffic accidents compete with falls for this position. TBI is the third most common injury to result from child abuse. Abuse causes 19% of cases of paediatric brain trauma, and the death rate is higher among these cases. Domestic violence is another cause of TBI, as are work-related and industrial accidents. Firearms and blast injuries from explosions are other causes of TBI, which is the leading cause of death and disability in war zones. According to Representative Bill Pascrell (Democrat, NJ), TBI is "the signature injury of the wars in Iraq and Afghanistan." There is a promising technology called activation database guided EEG biofeedback which has been documented to return a TBI's auditory memory ability to above the control group's performance.
Traumatic Brain Injury: Overview, In the Blink of an Eye
Uploaded on May 22, 2009
Brief overview of all videos that are part of the Be Smart. Be Well.TM TBI playlist. Experts touch on events that may lead to a traumatic brain injury and how to avoid it. Those who have been affected talk of their personal experiences.
A night out with friends changed Joshs life forever when a drunk driving accident left him with TBI. I woke up in a coma and dont remember much of the first year when I came home from the hospital. Watch and listen as Josh and his mom relive the accident and the times since.
Bicyclist Jerry sustained a TBI during a Sunday afternoon bike ride. I think the helmet saved my life because it was pretty smashed up, but that would have been my skull if it wasnt the helmet. See how his life changed.
Amy always dreamed of being a cheerleader when she grew up. But she never expected a cheerleading accident would lead to TBI. The most important thing for any survivor to know [is] that you really have to just believe in yourself and find inner strength in you. Learn what helped this former Miss Utah recover.