Lacunar Stroke From Wikipedia, the free encyclopedia.
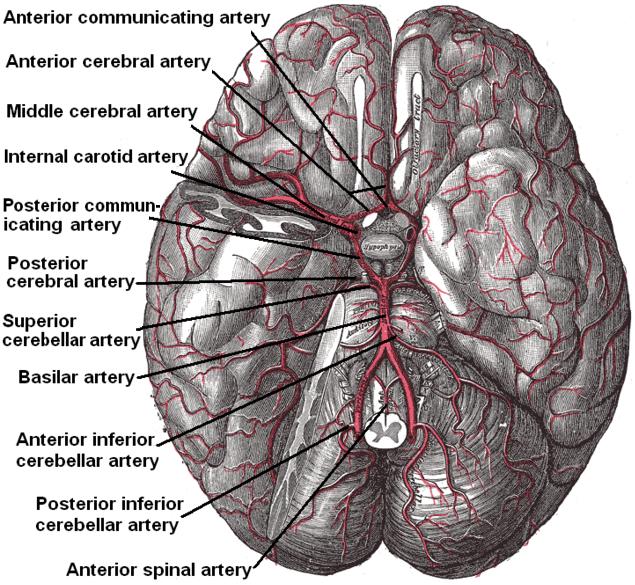
Lacunar Stroke - Arteries Beneath Brain
Much of the current knowledge of lacunar strokes comes from C. M. Fisher's cadaver dissections of post-mortem stroke patients. He observed "lacunes" (Latin for 'lake') of empty fluid left in the deep brain structures after occlusion of 200-800 μm penetrating arteries and connected them with 5 classic syndromes. These syndromes are still noted today, though lacunar infarcts are diagnosed based on clinical judgment and radiologic imaging.Epidemiology
It is estimated that lacunar infarcts account for 25% of all ischemic strokes, with an annual incidence of approximately 15 per 100,000 people. They may be more frequent in men and in people of African, Mexican, and Hong Kong Chinese descent.
Pathophysiology
Lacunes are caused by occlusion of a single deep penetrating artery that arises directly from the constituents of the Circle of Willis, cerebellar arteries, and basilar artery. The corresponding lesions occur in the deep nuclei of the brain (37% putamen, 14% thalamus, and 10% caudate) as well as the pons (16%) or the posterior limb of the internal capsule (10%). They occur less commonly in the deep cerebral white matter, the anterior limb of the internal capsule, and the cerebellum.
The two proposed mechanisms are microatheroma and lipohyalinosis. At the beginning, lipohyalinosis was thought to be the main small vessel pathology, but microatheroma now is thought to be the most common mechanism of arterial occlusion (or stenosis). Occasionally, atheroma in the parent artery blocks the orifice of the penetrating artery (luminal atheroma), or atheroma involves the origin of the penetrating artery (junctional atheroma). Alternatively, hypoperfusion is believed to be the mechanism when there is stenosis of the penetrating artery. When no evidence of small vessel disease is found on histologic examination, an embolic cause is assumed, either artery-to-artery embolism or cardioembolism. In one recent series, 25% of patients with clinical radiologically defined lacunes had a potential cardiac cause for their strokes.
Advanced age, chronic hypertension, smoking and diabetes mellitus are risk factors. It is unclear whether there is an association with alcohol consumption, elevated cholesterol, or history of prior stroke. Lacunar strokes may result from carotid artery pathology or microemboli from the heart as in atrial fibrillation. Patients often recover well, but if there is enough white matter disease from lacunar pathology, one can see a subcortical dementia such as Binswanger disease.
Silent Lacunar Infarction
A Silent lacunar infarction (SLI) is one type of silent stroke which usually shows no identifiable outward symptoms thus the term "silent". Individuals who suffer a SLI are often completely unaware they have suffered a stroke. This type of stroke often causes lesions in the surrounding brain tissue that are visibly detected via neuroimaging techniques such as MRI and computerized axial tomography (CT scan). Silent strokes, including silent lacunar infarctions, have been shown to be much more common than previously thought, with an estimated prevalence rate of eleven million per year in the United States. Approximately 10% of these silent strokes are silent lacunar infarctions. While dubbed "silent" due to the immediate lack of classic stroke symptoms, SLIs can cause damage to the surrounding brain tissue (lesions) and can affect various aspects of a persons mood, personality, and cognitive functioning. A SLI or any type of silent stroke places an individual at greater risk for future major stroke.
Treatment & Prognosis
Typically, tissue plasminogen activator may be administered within three hours of stroke onset if the patient is without contraindications (i.e. a bleeding diathesis such as recent major surgery or cancer with brain metastases). High dose aspirin can be given within 48 hours. For long term prevention of recurrence, medical regimens are typically aimed towards correcting the underlying risk factors for lacunar infarcts such as hypertension, diabetes mellitus and cigarette smoking. Blood thinners such as heparin and warfarin have shown no benefit over aspirin with regards to five year survival.
Patients who suffer lacunar strokes have a greater chance of surviving beyond thirty days (96%) than those with other types of stroke (85%), and better survival beyond a year (87% versus 65-70%). Between 70% and 80% are functionally independent at 1 year, compared with fewer than 50% otherwise.
Physiotherapy interventions are used in the rehabilitation of lacunar stroke. A physiotherapy program will improve joint range of motion of the paretic limb using passive range of motion exercises. When increases in activity are tolerated, and stability improvements are made, patients will progress from rolling to side-lying, to standing (with progressions to prone, quadruped, bridging, long-sitting and kneeling for example) and learn to transfer safely (from their bed to a chair or from a wheel chair to a car for example). Assistance and ambulation aids are used as required as the patient begins walking and lessened as function increases. Furthermore, splints and braces can be used to support limbs and joints to prevent complications such as contractures and spasticity. The rehabilitation healthcare team should also educate the patient and their family on common stroke symptoms and how to manage an onset of stroke. Continuing follow-up with a physician is essential so that the physician may monitor medication dosage and risk factors.
See the full article:
Lacunar Stroke from Wikipedia.
UW Medicine - Small Artery Stroke (Lacunar)
ProvidersKyra J. Becker, M.D. , Claire J. Creutzfeldt, M.D. , Vicki L. Johnson, D.N.P., MHSEd, A.R.N.P. , Sandeep P. Khot, M.D. , David L. Tirschwell, M.D., M.Sc. , Jonathan Richard Weinstein, M.D.
Overview
Small artery strokes are also ischemic strokes. These strokes are also called lacunar strokes. They are caused by blockage of one of the small arteries that branch off of the larger arteries. These small arteries penetrate deep into the brain, and can cause any of the symptoms of ischemic stroke. This type of stroke tends to have a better outcome, because the blockage of a smaller artery usually leads to a smaller amount of brain damage.
Once a small artery stroke has occurred, steps should be taken to help prevent further strokes.

See the full article Small Artery Stroke (Lacunar)
Brainstreams Strokes
- Ischemic, Hemorrhagic and Lacunar (3:07 - 4:10)
Strokes: Learn to distinguish between the different types of strokes including ischemic, hemorrhagic and lacunar. You can also learn about mini strokes or transient ischemic attacks (TIAs).
Standard YouTube License @ Brainstreams.ca Video Story Centre
Anatomy for Emergency Medicine #10 The Internal Capsule
from Andy Neill PLUS 1 year agoThere's a lot of common pathology in the internal capsule, both infarcts and bleeds. This covers the location and function and vascular supply of this area. Also distinguishes between a lacune, a lacunar infarct and a lacunar stroke. Life changing i know...
Emergency medicine doctor in Ireland. Doing a series of videos of anatomy specific to emergency medicine. External Links: http://emergencymedicineireland.com.
Anatomy for Emergency Medicine #10 The Internal Capsule from Andy Neill on Vimeo.
BRAIN MRI Multiple Lacunar Infarcts
Published on Apr 19, 2013Results:
MRI examination has been carried out head pieces axial, sagittal and coronal with T 1 WI and T 2 WI, slice thickness 10 mm without contrast Gd.DTPA with the following results:
- Lacuner lesions appear hypo intense on T1 and T2 in hiperintens the bilateral frontal lobes (12-14 pot slice axial, coronal slice 3-6 pots) and the left parietal lobe (12-14 pot slice axial, coronal slice pot 13-15).
- Sulci - sulci, fissures Sylvii, Cisterna basal, normal ambient Cisterna.
- Sistema ventricle within normal limits.
- Does not seem midline shift.
- Gray-white matter differentiation of normal.
- Normal brainstem and cerebellum.
- Cerebellopontine angle well, did not seem masses.
- Hypophyse not visible mass.
- Looks maxillaries sinus mucosal thickening in the left, and the left concha hyperthropy.
- Sinus spenoidalis, ethmoidalis, maxillary and frontal dextra not seem perselubungan. Mastoid air cells in the normal range, does not seem perselubungan.
- Bulbus oculi, m right-left rectus bulbi lateromedial normal, no lesion / mass in the region and ekstraconal intraconal. N. optici within normal limits.
Impression:
Multiple lacunar infarcts in bilateral frontal lobe and the left parietal lobe Sinusitis maxillaries the left with the left concha hyperthropi.
Standard YouTube License @ Umar Said
Lakshmi Neuro Center - Gait Training
A 60 year old man presented about 5 months after a left lacunar stroke. He had difficulty walking with a tendency to fall repeatedly. On examination, he had a circumdected gait with significant instability.He was put on a gait training programme. The focus was initially on teaching flexion at the hip and knee. The patient improved with appropriate therapy. After 6 weeks, he was able to walk with minimal support. He was also walking independently with a cane.
Standard YouTube License @ lakshmineurocentre
Francis Jones from Australia - Lacunar Infarction
Uploaded on Dec 7, 2011SSTattler: Poor video and questionable stem cell. You can read it for your own discretion.
In 2007, Francis was diagnosed with a lacunar infarction. There was skin damage and pigmentation on the lower limbs and he had a hemiplegic gait. The left side of his body had lost some movement and increased in tension. Only one month after Stem Cell Treatment, Francis has improved movement in his left arm. He can bend the elbow joint by himself and has a reduction in tension along his left side. He looks forward to further improvements over the following 6 months.
Standard YouTube License @ WSCMCindonesia
SSTattler: Lacunar Stroke Rehab - We will include total YouTube Part 1 through Part 5 and the Summary. Part 1, Part 5, Summary is the most important and Part 2,3,4 you can view them if you want to.
Lacunar Stroke Rehab Week 6 Part 1 of 5
Part 1 Includes an Intro and Leg Exercises.
Uploaded on Jun 7, 2010
Jack Schwenderman: Six weeks after suffering a Lacunar Infarction that left my entire right side paralyzed. Demonstration of progress made and current rehab exercises.
Standard YouTube License @ Jack Schwenderman
Lacunar Stroke Rehab Week 6 Part 2 of 5
Part 2 Includes More Leg Exercises.
Uploaded on Jun 7, 2010Standard YouTube License @ Jack Schwenderman
Lacunar Stroke Rehab Week 6 Part 3 of 5
Part 3 Includes Arm and Hand Exercises.
Uploaded on Jun 7, 2010
Standard YouTube License @ Jack Schwenderman
Lacunar Stroke Rehab Week 6 Part 4 of 5
Part 4 Includes More Arm and Hand Exercises.
Uploaded on Jun 7, 2010
Standard YouTube License @ Jack Schwenderman
Lacunar Stroke Rehab Week 6 Part 5 of 5
Part 5 Includes Stairs, Walking, and Wrap-Up.
Uploaded on Jun 7, 2010
Standard YouTube License @ Jack Schwenderman
Summary: Lacunar Stroke Rehab Week 16
Uploaded on Dec 26, 2011Some Comments (see all of them by Jack Schwenderman Videos) :
infark1 How about your condition now, I also have infarct in march 2012 with left paralysed in my left body arm and leg but now, my condition like your condition 16 weeks. are you already full recovery now, you already walk normally iasn't it?
Jack Schwenderman I will never be as good as before the stroke but I am doing fine. I am back at work fulltime (software engineer) and I can walk acouple miles. I have quite a limp and I use a Bioness L300 to assist with my foot drop. My hand is also not what it used to be. My finger flexer muscles overpower the extensors so I get Botox injections every 3 months. When the Botox kicks in my hand is fully open and pretty relaxed.
The strength is fairly week, but I can grasp and hold things. I can zip zippers and slice tomatoes, but not flip coins. My left is getting really good, so overall its not a bad way to come out of something so horrific. Thank you for asking!! I wish you all the best in your recovery. It takes time. Never give up.
Loretta Cannon I wanted to know if you have feeling in your right side at all? I had a left hemisphere stroke and I can not feel anything on my right side but I have pain in the left side of my leg when I walk.it always feels like it is cramping and I have to lean on something for a min.I think you are doing a great job and thank you for doing this.
Jack Schwenderman I do have feeling on my week side. It's a little off from normal, a bit numb-like, but not bad at all. At first I had no feeling on the right side but within the first 2 months it started to come back. I now can tell how much weight I have on each leg. My foot gets very cold at times due to less movement in the toes. My stroke happened in April 2010. Improvements for me have been slow but steady. I have had major setbacks caused by cold, damp winter weather. The lesson is to keep at it.
Standard YouTube License @ Jack Schwenderman