
Receptive Aphasia From Wikipedia,
the free encyclopedia
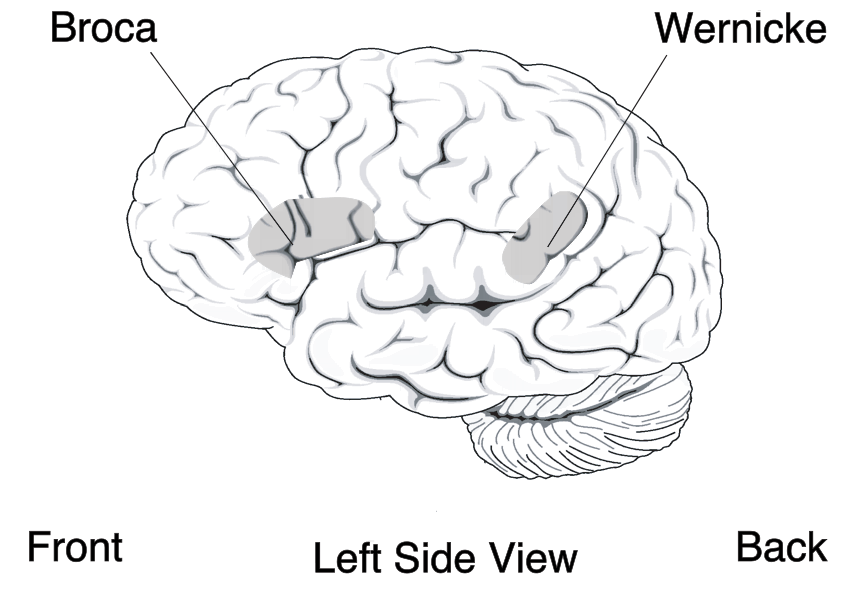 |
| Receptive aphasia Broca's area and Wernicke's area |
Receptive aphasia is not to be confused with Wernicke-Korsakoff syndrome.
Presentation
Two cortical areas central for the understanding and production of language are Wernicke’s area, and Broca’s area. Wernicke’s Area is located posterior to the lateral sulcus, typically in the left hemisphere, between the visual, auditory, and somesthetic areas of the cerebral cortex. A person with this aphasia speaks with normal prosody and intonation but uses random or invented words; leaves out key words; substitutes words or verb tenses, pronouns, or prepositions; and utters sentences that do not make sense. Therefore, their expressive language is devoid of any meaning. This is referred to as empty speech. Other symptoms can include a loss of verbal pragmatic skills and conversational turn-taking. As a result, these individuals often display logorrhea, a nonstop output of speech. A person with this aphasia cannot understand the spoken words of others or read written words. Speech is preserved, but language content is incorrect. Substitutions of one word for another (paraphasias, e.g. “telephone” for “television”) are common. Comprehension and repetition are poor.
Patients who recover from Wernicke’s aphasia report that, while aphasic, they found the speech of others to be unintelligible. And, despite being cognizant of the fact that they were speaking, they could neither stop themselves nor understand their own words.
The ability to understand and repeat songs is usually unaffected, as these are processed by the opposite hemisphere.
Patients also generally have no trouble purposefully reciting anything they have memorized. The ability to utter profanity is also left unaffected, however the patient typically has no control over it, and may not even understand their own profanity.
Damage to the posterior portion of the left hemisphere’s superior and middle temporal lobe or gyrus and the temporoparietal cortex can produce a lesion to Wernicke’s area and may cause fluent aphasia, or Wernicke’s aphasia. If Wernicke’s area is damaged in the non-dominant hemisphere, the syndrome resulting will be sensory dysprosody — the inability to perceive the pitch, rhythm, and emotional tone of speech.
Patients who communicated using sign language before the onset of the aphasia experience analogous symptoms.
Causes
Receptive aphasia is traditionally associated with neurological damage to Wernicke’s area in the brain, (Brodmann area 22, in the posterior part of the superior temporal gyrus of the dominant hemisphere). However, the key deficits of receptive aphasia do not come from damage to Wernicke's area; instead, most of the core difficulties are proposed to come from damage to the medial temporal lobe and underlying white matter. Wernicke's aphasia results from damage in the posterior one-third of the superior gyrus of the temporal lobe of the left hemisphere. Damage in this area not only destroys local language regions but also cuts off most of the occipital, temporal, and parietal regions from the core language region.
Luria's Theory
Luria proposed that this type of aphasia has three characteristics.
- A deficit in the categorization of sounds. In order to hear and understand what is said, one must be able to recognize the different sounds of spoken language. For example, hearing the difference between bad and bed is easy for native English speakers. The Dutch language however, makes a much greater difference in pronunciation between these vowels, and therefore the Dutch have difficulties hearing the difference between them in English pronunciation. This problem is exactly what patients with Wernicke’s aphasia have in their own language: they can't isolate significant sound characteristics and classify them into known meaningful systems.
- A defect in speech. A patient with Wernicke's aphasia can and may speak a great deal, but he or she confuses sound characteristics, producing “word salad” in extreme cases: intelligible words that appear to be strung together randomly.
- An impairment in writing. A person who cannot discern sounds cannot be expected to write.
See the full article:
Receptive Aphasia From Wikipedia, the free encyclopedia
No comments:
Post a Comment